Group’s improper accreditation could cost Virginia more than $11 million.
RICHMOND-A mistake by the Commonwealth Center for Children and Adolescents (CCCA) could cost Virginia more than $11 million. CCCA is a 48-bed mental health facility located in Staunton. Last year, the center served 1,079 children. In 2020, that number was near 1,000. The Virginia Department of Medical Assistance Services (DMAS) labels CCCA as a psychiatric hospital, and it does provide essential psychiatric services to young Virginians. However, the facility is accredited as a behavioral health organization, and has been since 1990. CCCA officials thought such an accreditation was sufficient to bill Medicaid for the services it provided, but recently discovered their error.
During its last session, the Virginia General Assembly convened a Children’s Inpatient Services Workgroup that uncovered the incongruity.
The U.S. Department of Health and Human Services requires that all DMAS facilities be “Medicare certified” or accredited as a psychiatric hospital with The Joint Commission. If the facilities, such as CCCA, are not properly accredited, they can’t be enrolled with DMAS. And that’s important because DMAS administers Medicaid services.
Virginia Department of Behavioral Health and Developmental Services (DBHDS) Commissioner Alison Land explained the problem to the Joint Subcommittee on Mental Health Services in the 21st Century during its meeting Dec. 21.
The department has a plan to make CCCA compliant with federal regulations. If it fails to do so, however, the state government may be liable for bills it improperly processed. Virginia may also be on the hook for between $11 and 20 million in repayments to the federal government.
Who Pays for Medicaid?
In describing the accreditation snafu to the subcommittee on Monday, Land called the situation “pretty critical, because those are the only pediatric beds we have.” In other words, CCCA is located in Central Virginia, but it’s a resource for children struggling with their mental health from around the state. It’s the only resource they have.
Children must be pre-screened for admission to CCCA by a community health board, which decides whether the child is “in crisis” in their current environment. If so, CCCA can provide support for children who have threatened or attempted suicide; displayed aggressive or assaultive behavior or exhibited a need for evaluation and medication management.
According to DBHDS Chief Public Relations Officer Meghan McGuire, approximately 60% of CCCA patients are Medicaid-eligible upon admission for a temporary detention order.
These children come from low-income backgrounds. Medicaid is a program funded jointly by the state and federal government to ensure people without sufficient financial means can still access necessary medical care.
Since 1990, Virginia has been contributing 50% to the cost-share for Medicaid patients at CCCA. The federal government covered the other 50%. Now, since it appears CCCA was not properly accredited as a Medicaid enrollee, legislators are wondering whether the federal government’s half needs to be paid back.
According to Land, CCCA stopped billing Medicaid on June 2, 2020. The group notified the Centers for Medicare and Medicaid Services of the issue on Dec. 14. DBHDS has a 12-month plan to address the accreditation issue and potential revenue shortfalls. If needed, DMAS will be working with federal regulators to pay back money owed. That money will be due by Dec. 14, 2021.
Mental Health Services Budget Already Slashed
Luckily, while DBHDS sorts out the paperwork, there will be no interruption of services at CCCA. “We were doing an inpatient, acute level of care at CCCA and continue to do that, so we just need to get this right from a billing perspective,” Land said during Monday’s subcommittee meeting.
However, CCCA predicts a $2.8 million revenue shortfall from the 12-month suspension in Medicaid billing. The accreditation process itself will also cost nearly $1 million. The facility will spend $718,000 on one-time capital improvements and operational modifications to meet requirements of a psychiatric hospital. It will also hire two staff members at a cost of $170,000 to guide the process. Land said DBHDS will absorb these staffing costs within its existing operating plan.
All these additional expenses come in a context of funding for mental health services being reduced dramatically in the past year. Multiple departments saw budgets cut due to the pandemic. State Senate Finance Committee Legislative Analyst Mike Tweedy explained these cuts during Monday’s meeting.
In the governor’s proposed 2021 budget, he removed $442 million from the state’s Department of Health and Human Resources. The General Assembly restored $224 million during the special session, but that still represents a $218 million cut. Specifically, community-based mental health services saw more than $52 million cut, Tweedy said.
Many of the programs that the joint subcommittee listed as top priorities during its last meeting on Dec. 9 were among those facing budget cuts. These included jail diversion programs, pilot programs to discharge geriatric patients with dementia from state mental health hospitals and the STEP-Virginia program.
Future of Deeds Commission in Virginia
The Joint Subcommittee on Mental Health Services in the 21st Century wants to restructure the mental healthcare system in Virginia. It’s been working as part of the Deeds Commission to fulfill that goal for seven years. But next year, the Deeds Commission expires.
So during the Dec. 21 meeting, legislators on the call also discussed what comes next for the subcommittee. The consensus was that the work needs to continue, but finding funding for staff the subcommittee needs is a primary obstacle.
“Four years is great, but you know, the work goes on forever. This is not an easy subject, and that’s because it’s complex and the issues constantly have to be considered and reconsidered to get the right approach,” said Sen. Creigh Deeds (D-Charlottesville), for whom the commission is named.
After some discussion, Del. Marcia Price (D-Newport News) made a motion to extend the commission for one year and to revisit the question of sustainable funding in the future. The motion passed.
Ashley Spinks Dugan is a freelance reporter for Dogwood. You can reach her at info@vadogwood.com.
DUBUQUE, Iowa. (KWWL) —– It’s Wednesday night, December 23rd, 2020. Two days ago, leadership in the U.S. House and Senate passed a coronavirus relief bill. Americans are waiting for details of long-awaited relief to be cemented.
For the Marshallese community, the wait for relief has lasted over 20 years.
Maitha Jolet is a Marshallese man living in Dubuque. He’s been watching national cable news, wishing for the moment the bill passes.
“[The pandemic] is really hard for the Marshallese community,” said Jolet.
Within the federal COVID-19 relief bill text, a proposal: restoring Medicaid eligibility for the roughly 30,000 migrants from the Marshall Islands who now live in the States.
U.S. troops took control of the Islands from the Axis powers near the end of World War II. U.S. nuclear testing started after the war, forcing migrants out.
Doctors think the testing resulted in staggeringly high rates of pre-existing conditions, including diabetes and heart disease.
This puts Islanders at extremely high risk for COVID-19 complications. Marshallese people make up less than 1% of the county’s population. By summertime, more than 20% of the county’s COVID-19 deaths were among Marshallese.
The community reacted, working fast with outreach groups, physicians and translators to get Marshallese connected to the care they needed, according to Kelly Larson, director for Dubuque’s Human Rights department.
“Pre-existing conditions — things that people from the Marshall Islands experience —- come from us having bombed their islands,” Larson said.
A pact between these Pacific islands and the U.S. (called COFA) gave the Marshallese the freedom to live and work in the U.S. In return, the States could sustain military presence there.
In 1986, the U.S. promised migrants eligbility for Medicaid coverage. Then, when Medicaid was reformed in 1996, the promise was broken.
Maitha Jolet
Jolet hopes the decades-long struggle will end soon.
“The government still owes people for what has been done,” Jolet said. “One of my friends’ wife, she died from the COVID. And he showed me the bill. The bill is around $114,000.”
“Something is not right. We are in poverty. We don’t have money.”
Two days before Christmas, Jolet waits with all of us for relief to be certain.
TennCare, Tennessee’s state Medicaid health plan, recently notified 3,300 members that their protected health information may have been exposed due to a misaddressed mailing incident on behalf of its vendor, according to a Dec. 21 WKRN report.
Gainwell, which runs the state’s Medicaid Management Information System, alerted TennCare of the breach in October. An investigation of the incident found that about 3,300 mailings sent out in late 2019 and 2020 may have been misaddressed and delivered to the wrong person.
The mailings, managed by the state’s vendor Axis Direct, contained protected health information of TennCare members. In a statement to the network, Gainwell said it is not aware of any members’ personal information having been misused as a result of the incident. The state is now offering free credit monitoring to the impacted members.
“TennCare is committed to safeguarding the information of our members. We have confidence in Gainwell and the process undertaken to identify the error that impacted certain members and correct it,” said TennCare Director Stephen Smith, according to the report.
Behavioral health and long-term care Medicaid reimbursement rate increases are set to go into effect on Jan. 1.. They were initially set to go into effect on July 1. The rate increases were passed through legislation in 2019.
Governor Larry Hogan announced the change on Thursday. Reimbursement rates will affect private health care providers who provide services to Marylanders on Medicaid.
Get the latest state-specific policy intelligence for the health care sector delivered to your inbox.
The changes to long-term care reimbursement will include nursing facilities, Rare and Expensive Case Management (REM), Development Disabilities Administration (DDA) targeted case management for certain individuals and private duty nursing. The Medicaid reimbursement rate for each will increase by 4 percent.
Behavioral health programs included in the bill will see a 3.5 percent increase in reimbursement. This includes behavioral analysis, adult residential and community-based substance use disorder treatment (SUD), mental health services, behavioral health targeted case management for children and adults, the 1915i community-based services program and therapeutic behavioral services.
The costs associated with the changes will be split between the state’s general funds and federal Medicaid funding.
Tennessee officials are hoping to get a response soon from the federal government regarding the state’s year-old request for a block grant waiver from the Centers for Medicare and Medicaid Services.
The proposal would amend the way the state distributes its Medicaid dollars through the TennCare program.
In November 2019, Tennessee became the first state to submit a block grant waiver to the federal authority under a new law approved by the state General Assembly.
State Sen. Rusty Crowe, R-Johnson City, said under this amendment, Tennessee is asking to convert the federal share of its Medicaid funding, which totals more than $7.9 billion annually, into a block grant to “provide core medical” services under TennCare.
“The goal is to provide the state an opportunity to address the specific health care needs of all Tennesseans, while lowering costs and increasing access to patient-centered care,” said Crowe, who presides as chairman of the state Senate Health and Welfare Committee.
If an agreement is reached between the state and federal governments on the waiver, Crowe said the plan will come back to Tennessee lawmakers for a final vote during the 2021 legislative session. The 112th session of the state General Assembly is scheduled to convene on Jan. 12.
Repub-licans, who hold a supermajority in the General Assembly, say the waiver gives Tennessee more flexibility to supervise its Medicaid programs while also providing the state with an opportunity to rein in spending.
“Tennessee has completely different health care needs across its nearly 500-mile span,” state Sen. Jon Lundberg, R-Bristol, said Tuesday. “This will give us a better opportunity to disperse those Medicaid dollars to meet those needs.”
Lundberg said the state officials are hoping to hear word of the waiver before President Donald Trump leaves office.
“We really don’t know how the new administration will react,” Lundberg said.
Officials say approval of the Medicaid waiver has been delayed as federal authorities have asked the state for more details to clarify the proposal.
In the meantime, recommendations from a legislative panel appointed to study possible changes to the state’s Temporary Assistance to Needy Families Program is expected to be considered by the General Assembly in 2021. Tennessee has $741 million in unspent funds from the federal block grant program that supports Tennessee’s Families First program.
Families First provides support to Tennessee families in need of child care assistance, temporary cash assistance, transportation and job training.
“Discussions on how to best allocate the unspent funds were interrupted by COVID-19 last session,” Crowe said.
The Johnson City senator said he will sponsor legislation to require the state’s Department of Human Services submit an annual report to the General Assembly that includes information pertaining to TANF program. Crowe said that report would give details of organizations receiving TANF funds, and how recipients are spending those dollars.
The author of this Forbes op-ed argues that ACA underprojections and the rich FMAP for expansion enrollees has created a moral hazard for state programs that results in disadvantaging disabled Medicaid enrollees.
The article below has been highlighted and summarized by our research team. It is provided here for member convenience as part of our Curator service.
The question before the high court is a legal one. But as a matter of policy, work requirements are a great way to rein in Medicaid’s out-of-control spending and preserve the program’s scarce resources for the truly needy.
Several states—including Kentucky, Arkansas, and New Hampshire—have pondered work requirements in hopes of limiting Medicaid enrollment, which has exploded in recent years. The program was created more than a half-century ago to provide health insurance to the poor, disabled, and pregnant women. But as of July, it covered nearly 69 million people. That’s roughly one in five Americans.
Many states thought expanding Medicaid would be a great deal. After all, Obamacare bound the federal government to pay 90% of the cost of covering the expansion population.
Even with that hefty assist, several states are struggling with their Medicaid tab.
For starters, many more people have signed up than the states projected. In 2017, the Foundation for Government Accountability investigated enrollment of the expansion population in 24 states as of 2015 and 2016—and found that it was more than double what the states expected.
Medicaid has long been the 800-pound gorilla in state budgets. States cover a little over one-third of the more than $600 billion the country spends on the program each year. Together, Medicaid and the related Children’s Health Insurance Program account for nearly 30% of state spending. They’re the second-largest line item in state budgets.
Every dollar that goes toward a new, able-bodied Medicaid beneficiary is a dollar that can’t go toward other state responsibilities like public safety or infrastructure.
And thanks to the pandemic-induced economic downturn, those tax dollars are harder to come by. According to a Kaiser Family Foundation survey, 17 of 19 states with budget projections for 2021 reported a Medicaid budget shortfall was “nearly certain” or “likely.”
Work requirements can help states preserve their Medicaid resources for the program’s original beneficiaries—the impoverished and disabled—by nudging the able-bodied on the path to self-sufficiency. Research from the Buckeye Institute has found that work requirements can increase lifetime earnings close to $1 million for individuals who eventually transition off Medicaid.
It’s far better for taxpayers—and would-be Medicaid beneficiaries themselves—to get insurance through their jobs or to accumulate enough income to pay for coverage on their own.
Further, by tightening eligibility for the program, work requirements can make it easy for the program’s legacy beneficiaries to secure care.
Medicaid pays doctors and hospitals less than Medicare or private insurance. So healthcare providers often limit the number of Medicaid patients they’ll see. About 70% of providers accept Medicaid, according to a national survey from 2015. Eighty-five percent accept Medicare, and 90% private insurance.
Expanding Medicaid has created additional competition for scarce appointments. That can mean legacy beneficiaries have to wait longer than they would have pre-Obamacare.
States’ limited resources—and the higher payments they receive from the federal government for expansion enrollees—can cause them to de-emphasize the needs of disabled enrollees, for whom they bear more of the cost. A study from the Foundation for Government Accountability found that nearly 250,000 disabled individuals were on waiting lists for Medicaid care as of 2016 in states that had expanded the program to able-bodied people.
Other government programs for the poor, like the Supplemental Nutrition Assistance Program and Temporary Assistance for Needy Families, have employed work requirements with great success. When the Clinton administration required single parents to work or seek work to receive TANF, childhood poverty plummeted, and employment soared in the years that followed.
Medicaid was created to help the needy, not those who should be able to take care of themselves. Requiring able-bodied adults to seek employment in exchange for taxpayer-funded health insurance shouldn’t be controversial. It should be common sense.
A federal Medicaid program is providing just more than $3 million in funding for the state’s early childhood program known as Reach Out and Read.
The program will be conducted by the N.C. Department of Health and Human Services with matching funds.
DHHS said the reading initiative is one of the first in the country among state Medicaid programs.
The goal is improving literacy and language comprehension through participation from low-income children who would be eligible for Medicaid or the federal Children’s Health Insurance Program
Meanwhile, the federal Centers for Medicare and Medicaid Services said the program has proven in other states to have improved patient-clinician relationships and well-child visit attendance.
“Expanding Reach Out and Read recognizes that children’s healthy development and early literacy are intertwined,” Dr. Mandy Cohen, the state’s health secretary, said in a statement.
“This program meets families where they are and through people they trust.”
Reach Out and Read partners with pediatric primary care locations to deliver training for medical providers, literacy tools for families, and to encourage healthy routines and relationships through shared stories.
CMS has begun the process to define value based purchasing arrangements for drugs in the Medicaid program, with a focus on the value delivered by a drug to the individual patient. One key change to regs is to allow manufacturers the ability to report multiple best prices.
The article below has been highlighted and summarized by our research team. It is provided here for member convenience as part of our Curator service.
New value-based pricing approaches could save up to $228 million in federal and state dollars through 2025.
The final rule codifies a broad definition of VBP, which can better align pricing and payment to observed or expected evidence and/or outcomes-based measures in a targeted population. (Image: Shutterstock)
States, private payers and manufacturers now have more flexibility to enter into value-based purchasing (VBP) arrangements for prescription drugs under Medicaid. The Centers for Medicare & Medicaid Services on Monday finalized regulatory changes to modernize Medicaid prescription drug purchasing and drive payment innovation.
“Rules on prescription drug rebates and related reporting requirements have not been updated in thirty years and are thwarting innovative payment models in the private sector,” CMS Administrator Seema Verma said. “Medicaid’s outdated rules have consistently stymied the ability of payers and manufacturers to negotiate drug reimbursement methods based on the actual outcome of the treatment. A new generation of approaches to payment methods is needed to allow the market the room to adapt to these types of curative treatments while ensuring that public programs like Medicaid remain sustainable and continue to receive their statutorily required discounts.”
Under current regulations, prescription drug manufacturers face challenges accounting for VBP arrangements in their Medicaid best price reporting to CMS. This has the unintended consequence of hindering providers, insurers and prescription drug manufacturers in their efforts to develop innovative payment models for new drug therapies and other innovative treatments. Current regulations also discourage payers and manufacturers from designing new payment arrangements based on the value their product may provide.
With the new flexibilities under this final rule, manufacturers are expected to be more willing to negotiate with payers, including Medicaid, with drug pricing being driven by the value of their drug to the individual patient. New genetic-based treatments initially may be expensive but in the long run offer significant value to the patient and payer.
Payers will be able to negotiate prices with manufacturers for these genetic-based treatments based upon outcomes and evidence-based measures such as reduced hospitalizations, lab visits and physician office visits, ensuring that if such measures fail to support the value of a drug, the payer is not held accountable for the full price.
The final rule codifies a broad definition of VBP, which can better align pricing and payment to observed or expected evidence and/or outcomes-based measures in a targeted population. The final rule also allows manufacturers to report multiple best prices instead of a single best price when offering their VBP arrangements to all states. By making these changes, effective in January 2022, CMS hopes to encourage VBP arrangements and negotiations to help make new, innovative therapies more available to all patients. As a result, it is estimated that these new
VBP approaches could save up to $228 million in federal and state dollars through 2025. Basing payment on the effectiveness of a given therapy can foster innovation in the treatments that are most beneficial to patients, while reducing overall health-care spending and hospital visits. When payers are positioned to be stronger negotiators with drug manufacturers, Medicaid beneficiaries will benefit from better access to prescription medications.
best viewed on a tablet, using quality headphones (if you can read and listen to music at the same time).
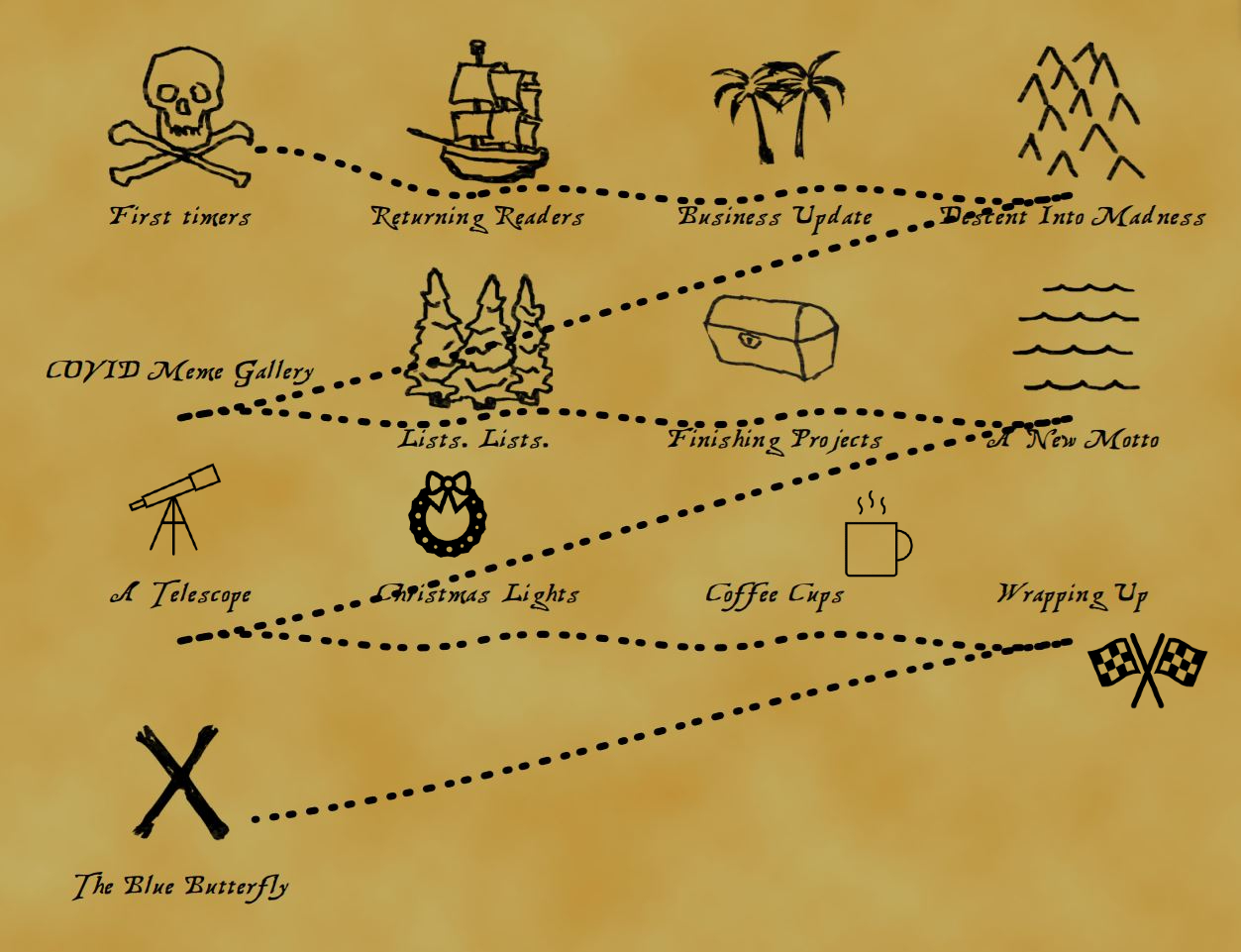
Here is your treasure map. You might want to take a look at it.
Hit play and start reading.
Whiskey Tango Foxtrot. End of review.
I guess I have to do better than that.
I have avoided writing this for about 2 months now. I think you can guess why. If the past Year in Reviews (YERs?) have been a beer to get you tipsy, this one is 4 hits of acid and a side of peyote. It’s rough. Heaven help us all as I try to look back and find meaning in this hellscape of a year.
I am sorry I meant to say this peaceful protest of a year.
Please don’t cancel me.
Or take away my adrenochrome or my goats. More on both of those later.
There were also giant blue butterflies. More on those later, too.
I promise the payout is worth it this year. Read it all the way to the end. There is that blue butterfly. But don’t skip to it because it will make no sense without all the rest.
If this is your first time to these Year in Reviews that I do
Here’s a guide:
I take a long time to wind up.
I cover a lot of ground, mostly in loosely connected glimpses into things that stuck out to me as meaningful duringthe year.
I attempt to stitch it all together with a metaphor that I introduce early, hide more and more throughout and then bring back to make the final pop both mentally and emotionally.
I will most likely make you mad.
I hope to make you think.
I will share the Gospel at some point, and if for any reason I forget to (which I doubt I will because I read these things over and over and over when editing), please call or email and ask me to share it with you. Whether or not you already believe. I love to tell the story.
If I do my job right, we all have a good laugh, a good cry, and feel human again at the very end.
P.S. Each Year in Review gets its own unique icon. This year’s candidates are:
Whenever you see the butterfly one, you can click on it to listen to a recommended soundtrack for the section. This will include and either a song I wrote or a song from someone else I think is appropriate in the context of the section.
P.P.S. This year’s review may end up making you feel worse than before you read it. Caveat Reador.
P.P.P.S. I am an extreme person. If I didn’t have a blackened heart before 2020, I certainly do now.
If you end up liking this (a surprising number of people do and that is scary / humbling), here are links to past reviews
Then you know all the stuff above, whether you realize it or not.
But this year is, of course, different. In other years, I sat down over several multi-hour sessions and poured out my mind and heart to my audience. This year its more like I am on a sidewalk in a deserted alley somewhere, vomiting on all fours with snot and tears and rage gushing out of me. You have been warned.
I have placed links throughout if you just need to hit the escape button and get lost in a great song or a related wiki entry or similar.
Oh yeah, the business
Are you a healthcare industry nerd? Join our team! It’s amazing. And this is literally the first thing you see as part of our New Team Member Onboarding Process.
For whatever weird reason, I have almost no distinction between my work and my life. Clients seem to like it because it makes healthcare consulting human. And genuine human-ness is loved by anyone remotely human. So clients become friends.
I always publish the YER out to the business site to hit both parts of my life, I guess. So I need to give everyone some business-ey updates first. Price-to-pay and all that. Then we can get back to the life stuff.
Maybe I’ll do a timeline.
January – February Brought on a new Partner and Chief Growth Officer. He is simply put the only person I would trust to run the business instead of me. He’s smart, thorough, kind and always learning. His name is Kris.
March– COVID started to be real. The HIMSS conference got cancelled and anyone who wasn’t yet woke to COVID in healthcare was now. Clients starting cancelling contracts.
April-ish– We seriously asked ourselves if we would be on the ropes in 6 months, decided we were ok with whatever happened and that we were going to give it our all either way. We pivoted completely into understanding how COVID was impacting our clients and audience. We called them up- human to human- to ask how they were doing. We did listening sessions with executives to hear what was important to them now in this new reality.
May– I said to the team “Hey- let’s do a four-day virtual conference all about Medicaid and COVID. It’ll be easy.” We pulled it off by mid-June and hundreds of people sat through 4 solid days of health plan CEOs, CMS officials and state Medicaid Directors discussing what they were doing about COVID. Sarai was absolutely amazing during all this (and actually ran the thing live for about an hour while I had a medical emergency during a speaker session).
June– August– Business picked up. New clients. New friends. All of sudden a lot bigger team. Building out a dream team of consultants is probably the best part of 2020 from a work side. And we made sure we thought about how to be human across our team. You haven’t lived until you’ve heard very important government officials talk about the dangers of crashing a Serbian wedding over Zoom happy hour.
Sept-October- Lots of fun and fulfillment delivering on all the stuff Kris sold. Getting to work with experts who were your heroes 15 years ago is an amazing thing. Started the newsletter back up.
November- Started working on spreading human-ness again back to the audience with the MegaMixTape project. People loved it.
December- Now on track for best year ever as business. Excited about what’s next. Planning our first real in-person conference. Theme: Humans. Or maybe hugs.
Ok, that’s it for the business update for 2020. Back to the reason you’re here.
Descent into madness
The soundtrack for this section includes 3 songs I wrote: 1) Ring the Bell: A song I wrote during the time of the events described below. Kind of serves as a nice score while reading the below if you are game for eerie electronic stuff. 2) End of the World– sad guitar stuff; and 3) Morning Coffee– If you need a little pick me up after all that, this is sort of like if you went to a jazz brunch and someone used coke instead of powdered sugar on your French toast. But pulled back the edge with a lot of Ginseng.
My wife was watching international news (she has a much more effective Twitter feed than I do for healthcare items, which is funny because I am the healthcare half of us.. but then again I guess the past 5 or 6 years being a complex auto-immune / blood disorder patient probably makes her pretty qualified in the “healthcare” bucket) and was asking me if I was “watching this Wuhan thing.”
“Nah,” said the guy with the public health degree from Johns Hopkins. “Probably no big deal.”
She continued to watch it develop and continued to nudge me on it, so that by early February I was asking colleagues in the healthcare industry- “Hey, are you watching this Wuhan thing?”
Their response- “Nah. Probably no big deal. Are you going to the HIMSS conference this year?”
I then realized even the people who should be watching this were not. And if they were not, then I was certain those in my social circle (non-healthcare people, friends and family) absolutely were not.
So in early March I dropped everything and pivoted 180 away from the healthcare industry and towards my social circle.
Late February and Early March
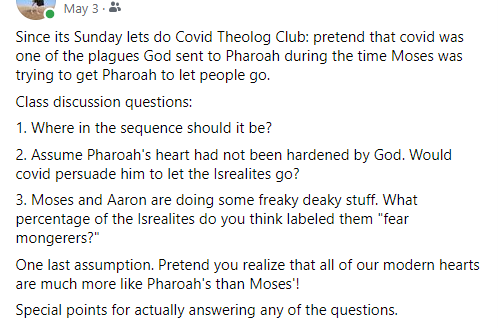
In which I believed educating people was the answer.
I went to Facebook to share as much information as I could. (Before this I might have gone on Facebook 3 times a year).
And what I found terrified me.
A solid majority of people I knew thought this was all a George-Soros funded hoax designed to unseat Trump.{1}
The “same as flu” crowd.
The “its 5g bats sending messages from cell towers on behalf of Bill Gates and the New World Order” crowd.
The “Q anon” cult.
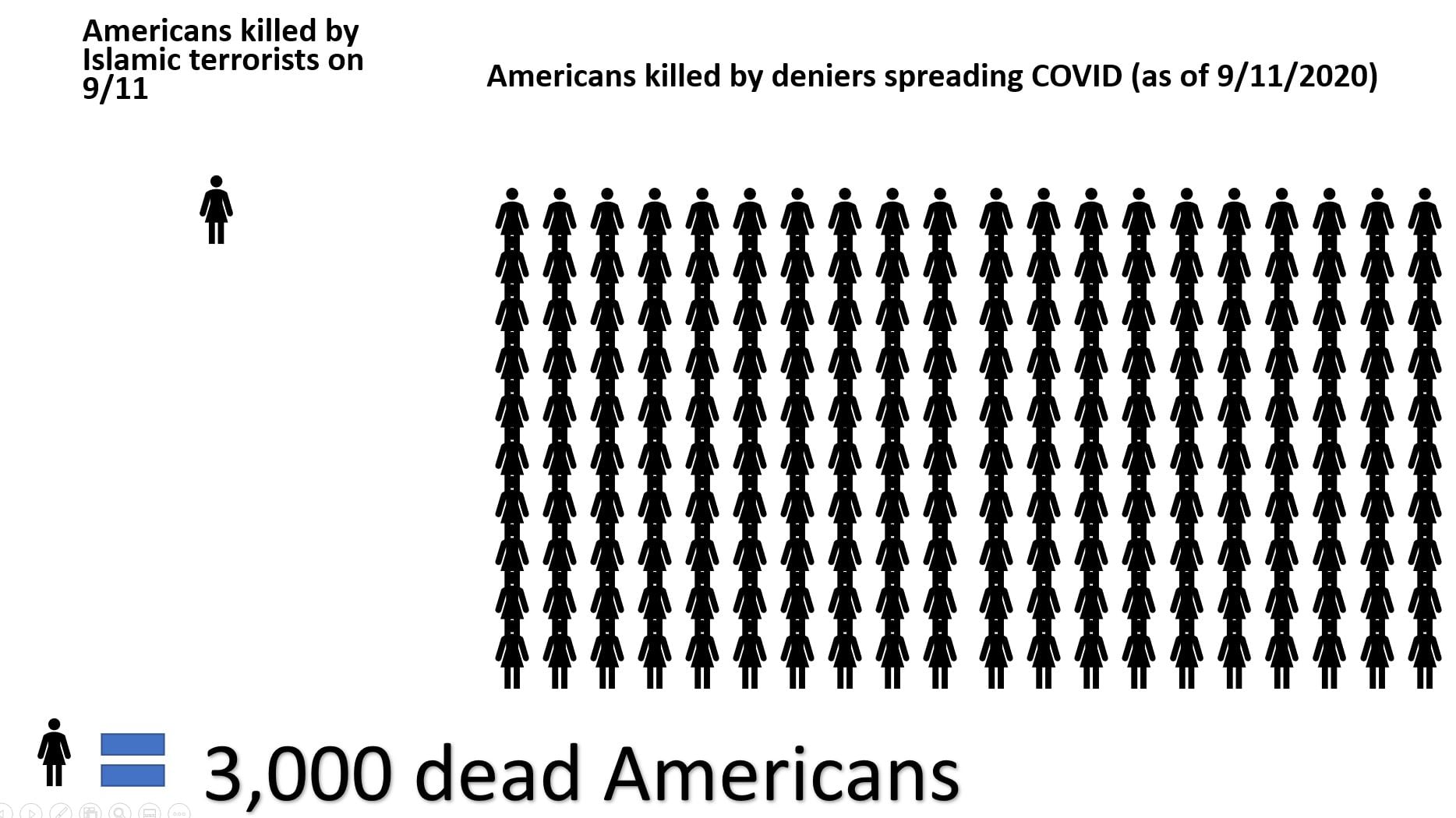
You know. The people who murdered 300,000 Americans (and counting) with their selfishness and their 2-standard-devs-to-the-left capabilities.
Those guys.
But in March, I had not yet realized how willfully ignorant about millions of Americans have become. I still thought “if only they could get some accurate information, translated in a way that laypersons can understand, they’ll make some hard adjustment to their lifestyle and we can be done with this in a month or so.”
That was where my head was at in March 2019.
This was basic infectious disease. Change a few small behaviors, stop the spread. Viruses stop when there are no more victim opportunities.
Forming (and informing)
Late March
But anyway. Back to before I gave up. In March I stood up a curation team.
I enlisted the support of people whose medical and public health opinion I trusted. Doctors in ERs in multiple states. Former (and current) state health and CMS officials. A DC press guy (you know who you are Mr. MFAR). The plan was simple. Text me any articles you think are helpful and I will get them out to my Facebook circle.
We called this Ringing the Bell.
It took off like wildfire.
Very quickly it got to the point where we needed more help. People reading all the stuff we were putting out and resharing it (dubbed “Bell Ringers”) needed help understanding it. So then we pulled in half a dozen or so doctors, psychiatrists, biochemists and public health professionals to explain and discuss (in the comments) the articles we were putting out.
To look back on this now, it is amazing that we were Ringing the Bell in this way. Getting out information that most people were not seeing anywhere else. And that has a lot to do with the bubbles and filters and knowledge ghettoes we build for ourselves with modern media. But that’s a whole other topic that I don’t have time to cover here.
We were Ringing the Fuck Out of the Bell until we got everyone’s attention. {2}
Pretty quickly I was organizing all the news stories of the day into sections (clinical, supply chain, social unrest, data..) and running a Facebook Live “news show” every night. At one point we had something like a hundred people watching it regularly.
I made our Facebook profile public to make sure we could get the word out. Stacy hated that but understood why. People from all over the country followed it. I would get phone calls from people I have never met asking me to help them think through whether to drive 12 hours to get their elderly parents so that they could quarantine with them. Or callers asking “What is a cytokine storm? Can I give my baby elderberry?”
I did my very best to answer and to explain what I did or didn’t know. I was completely humbled by them trusting me. And completely broken by the realization that this was how bad it was: people were blindsided by a cataclysmic, world-changing event without sufficient information for them to respond to it. So much so that they were calling a stranger across the country to ask for advice. All because some person they knew saw this guy on Facebook.
April
A bitter pill
It sucks to see things coming from further off than most everyone else. Bad things.
Remember we were way early in the deaths and even in the cases at this point. I would say things like:
“If there are 500 reported cases in Alabama, I promise there are really 10,000 running around out there.” Turns out that was probably pretty close.
Or when the CDC said on a Friday that 200 people indoors was safe, I would say that was nuts. And then on aSunday (two days later), when they dropped it down to 75- I’d say of course 76 is not safe. And so on and so forth.
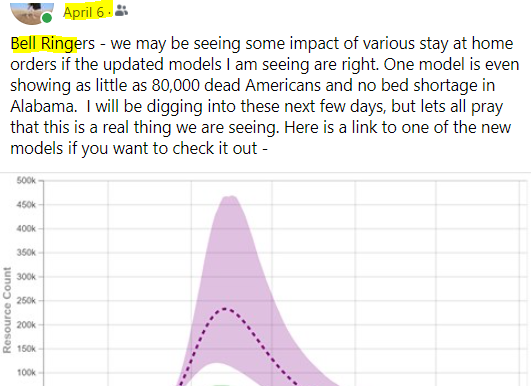
And when the Imperial College study came out showing peak American death in June for America around 2M dead, I spent hours explaining what that number really meant. And that Trump’s counter-number of 80,000 dead total was nonsense.
And when I told people we would have a completely divided country of over masks (in April), few listened.
When you are one of the few who is willing to read the clearly legible handwriting on the wall, its very lonely. And this is not one of the ones where later saying “I told you so!” has any joy to it at all.
I think it was in late April that I realized The Bell Had Been Rung. I began to pivot back into writing music. I began to try to find small ways to relate to the people I would interact with over the phone. Dealing with a pandemic from a business perspective involves a lot of phone calls. I remember praying for customer service representatives a lot during this time. One lady and I had a twenty-minute conversation about each of our wedding stories. She had taken a cruise for her honeymoon right before the COVID cruise ships happened.
Remember that? When cruise ships were trying to find a port that would let them in? Or what about the USS Comfort that went to NYC in the initial onslaught? So much has happened.
In the beginning I prayed over every UPS, USPS or Amazon driver I saw at the fence. Out loud. For their protection during this time. God used that to minister to them but also to me.
June to November
Retreat and Surrender
By June I was angry. Educating had not worked to change people’s behavior. And I am still seeing lots of pictures even now (December) of groups of people with no masks at Christmas parties.
Spreading death.
A pox on their houses.
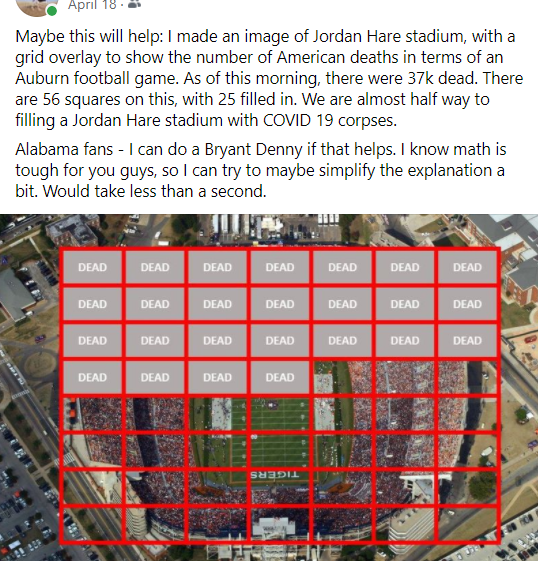
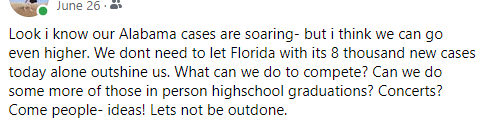
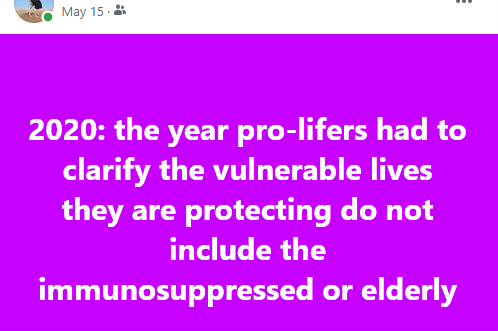
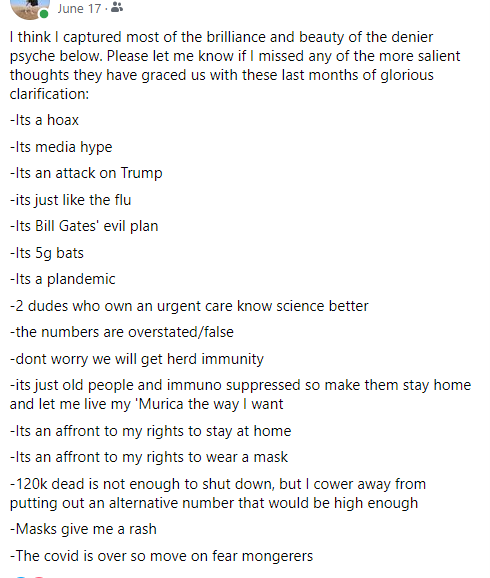
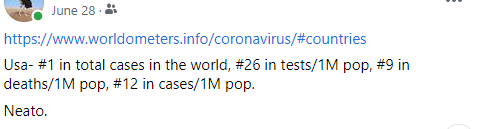
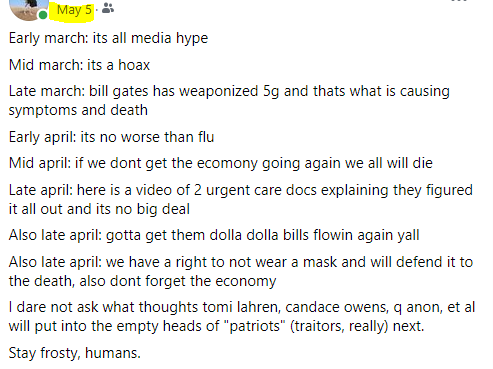
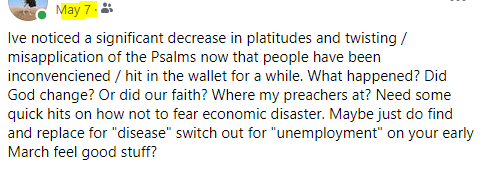
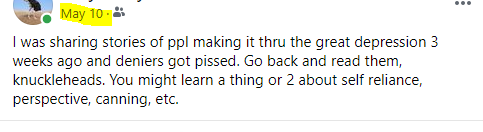
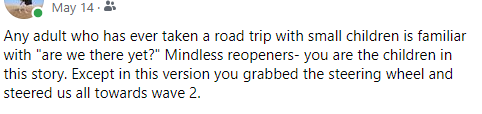
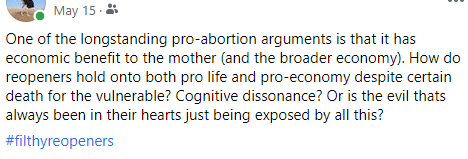
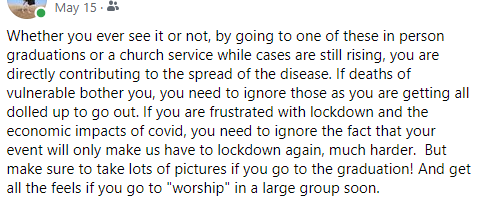
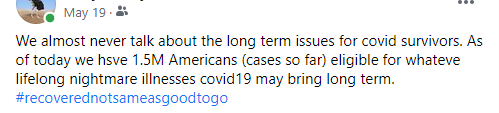
So I turned to memes. At first I put out a steady stream of them.
I do believe shame and guilt (but more so guilt) likely have more of a role to play in stopping this disease than we realize. Hell, maybe even more a role than the vaccine.
Instead of narrating all my meme adventures, I’ll just let you click through them in this slideshow below. I’m sure you’ll get the idea.
Lost more than a few friends over these. Made some new ones, too. Would do it all over again.
December
Remembering and Reflecting
But looking back at all this, I just don’t know what to make of it.
I had tried to warn people. To ring the bell. Many listened. More did not.
And it hurt me.
No. It broke me.
Most of the madness part is over. If you have been hiding behind the couch while the scary man screams, its ok to come out now.
Human Contact
As I sit down to write this (design started November 21- I always start these at least a month early) I have not hugged my momma in 250 days. She is still alive. She lives less than 5 miles from me. I have seen her many times in since March.
But I have not hugged her.
We have seen many friends and family during this time. In our yard. From 20 feet away. You see, we take this seriously. We don’t think that the tiny little exceptions we want to make ourselves (or someone else) happy are exceptions to the fundamental principles of infectious disease. So we have been home since March 12, 2019. And when I say home, I mean home. We go out for doctor’s visits (my immunosuppressed wife still needs those even while America parties). That’s it.
But anyway, back to March 12th.
That’s my youngest son’s birthday. And we celebrated it by eating icecream for dinner at Top It Off (a local icecream place). We lived it up. All 6 of us got all the fixins – sprinkles, gummy bears, heath bits, oreos, almonds. Whatever nasty combination each of us wanted, because I knew we would not be coming out again anytime soon.
And just when we had been getting into a good rhythm as a family going to eat Italian every Tuesday at Vecchias. Or the library twice a week. Or church. Or thrift stores.
I keep two lists (mentally) along these lines.
There are the lists of things I am heartbroken for my children about that COVID (and her helpers, Deniers and Downplayers) has taken away. Things like chess tournaments for Nora. Or any of them playing with their little friends. Or trips to visit Grandpa in his new house in Florida. Or the cross-country road trip we had planned for last April. (I was going to chair a dental conference in Arizona, of all things).
Then there is the list for my wife and I. When (or will?) my wife be able to go wander aimlessly through a thrift store for hours to veg out after a crazy week of homeschooling four kids? When will she be able to see her daddy again and hug him?
You keep different lists once you have kids and get married. The real lists are not for yourself.
I do have a list for me- full of stupid crap- similar to most of selfish America, I guess:
Will I see an opera again? (funny that’s something I COVID-pine for, even though I haven’t been to the opera in 20 years)
Or go out to eat at a restaurant and sit for hours?
Or go to another conference?
Or see another Auburn football game?
Or play an open mic night with my new guitar?
For me, there is only 1 thing on my list
When will I hug my momma again?
Lists. Lists.
So many lists
If I could boil down my biggest problem in life, and if I am honest (that’s always the hard part, right?) its that I compulsively write down lists all the time. Lists of ideas. Lists of tasks. Lists of things I want to do, lists of places I want to go. Lists of books I want to write. Lists of regrets. Lists of songs I want played at my funeral. Lists of lists.
Lists can be good. They can help you organize. They can pull things out of your head.
But for me they are shackles.
If it goes on a list, I feel it must be done. Someday. No matter how long it takes. It must be completed, or purchased, or replaced with something even better. I have lists I have kept for more than 10 years, and I still am compelled to try and complete them.
I use any productivity tool I can find. Evernote, OneNote. David Allen’s Getting Things Done.
I have a Kanban view on my entire life. I literally organize my life into numbered areas that are each statements meant to help me get un-lost while on my lists:
1-Clay Loves God
2-Clay Loves Stacy
3-Clay Loves the Kids
4- Clay Loves Friends and Family
5- Clay is Blessed With Work
6- Clay is Blessed With Resources
7- Clay is Blessed With Pursuits
And all the items on all the Lists go into one of those buckets.
Sometimes this is a good system.
When you need to get back on the wagon and get things done, it is very helpful to have a wholistic structure. You find your place and fall into line. Its easier to put one foot in front of the other when you at least have a general belief that where you put that next footstep is meaningful in some way.
And if you are a voracious reader/doer/maker, this is a very good system for organizing your thoughts and information needed to Complete Your Lists.
But sometimes even the best systems cannot keep it all on track. Sometimes you have to just make things with your hands and set the list down for a while.
It was helpful that I had a List of Unfinished Outdoor Projects once COVID hit.
Finishing up projects
another list
Remember in government school when we would come back from summer vacation and have to do a report of what we did over the break?
Here is the List of Things I Built This Summer:
Approximately 1,500 feet of wooden fence
A 200ftx200ft pen for the goats and ducks
Four 80-foot long irrigated beds in the garden
A completely organized workshop
A greenhouse
A new bedroom for my 12-year-old daughter for her birthday (needed to be a big birthday to try and distract from COVID)
A deck addition to the treehouse I built years ago
A chicken run and nesting box under the new treehouse deck to house our 7 (now 6) new chickens
A barn to house our 2 new goats, 5 old ducks and 2 new ones
A new system for growing plants in my basement (right now I am growing lavender, lupine, hyssop, chamomile, and parsley under grow lights)
A goat playground
A smaller pen for the goats near the barn for rainy days
A pond for the ducks (they are most happy on water)
An herb garden near the above ground pool
Oh yeah, a 20×20 foot box to handshovel roughly 15,000 pounds of sand into to put our new above ground pool on. We live on a slope so I needed to create “level.”
A “children’s garden” of three 12-foot long raised beds near the treehouse
A covered “loading dock” – which is a platform for delivery drivers to use
Lots of other smaller projects, and I’m sure a few major ones that I just forgot
I’d like to say that these all were finished in an orderly fashion. Each one done before moving onto the next. But they were not.
For the longest time, our 2 little acres of heaven sat strewn with piles of building materials as I bounced unfocused-ly from one project to the next.
When times get tough, I build things.
And when I realized the benefit of Building Things As Therapy, I went all in. Or aller-in. I was already pretty crazy about it. And it of course got me in good shape. Digging hundreds of post holes and shoveling tons of material will do that.
You should see my National Naked Gardening Day photos (I put those on Facebook). I looked amazing. And happy.
What happens when you click this image? (2021’s NNGD will be May 2nd, by the way).
Time for a music break? Maybe listen to these 2 before Pushing Through. (Many people can’t read and listen to music at the same time). Or maybe later…
Grasping for a new motto
As you know (if you have been here before), I try to suss out some sort of congealed truth in these YERs. And then I fashion it into a motto for the next year.
I am struggling to find the motto for 2021. I just can’t get myself to believe the locusts have stopped eating. Underneath it all, I think I fear 2020 and 2021 will be sandwiched together, distinguishable only by their peaks and valleys.
Two people on a zoom Christmas party in 2021:
“Remember that month in 2020 where we only had a few hundred deaths a day and not 2,000?”
“Yeah, that was great. Had one of those in 2021, right? March, maybe?”
COVID infects both our brain and our bodies. All our souls are in a supernatural ICU right now, choking and sputtering. Staring at the hospital walls wondering when (or if) we will get better. It has robbed us of so much that its hard to see what remains. Or even remember what was there before.
I wanted so badly to make the 2021 motto be “Pushing Through.” Its something Daddy used to say. He’d say “son, when you’re in those dark clouds- just keeping pushing through. You’ll get through it eventually.”
But eventually has become a lost year. The clouds are more than 300,000 dead Americans. Or a nation of Deniers and Downplayers who dishonor those dead by continuing to go to gatherings.
These are some dark clouds, Daddy.
I miss you so much and I want your words to still work on this one. But I just don’t think they will.
Straining to see the light
New motto?
I finally got a telescope for the kids this year. Well for me, really. I think this is something middle-aged dads do. I can remember a dad of a friend of mine doing this 20 years ago. Jimmy bought an amazing telescope (he spent money on toys and man was it worth it to be around him. Guitars, a new jeep. Telescopes). And he also leased this 10×10 spot on top of a mountain in Alabama where a hundred or so other stargazers would go on winter nights to look at those burning lights so far away.
I am now the same age Jimmy was when I met him. This amazes me.
Jimmy, I know there is almost zero chance you are reading this. But if you are, I want you to know you were a good dad. And not just to your own kids. Thank you for doing cool things with us. You absolutely got that part 100% right.
But back to my telescope. I mean the kids’ telescope.
We all have this idea that we can work a telescope. Point it at the sky when there are tons of stars. Turn a few dials and voila, each of us is Galileo.
Seems easy, right?
Not so, friends. Not so.
Putting it together is easy enough. But then you get to the lenses and eyepieces. And you realize you have no idea what a Barlow lens is. Or whether the 10mm or 25mm one is better.
You just want to point that thing at stellar awesomeness and call the kids over and let the magic happen.
Turns out magic takes learning some new skills.
Lesson 1- find the darkest part of your yard. Standing next to your living room window with the lights on inside the house is not optimal.
Lesson 2- learn the difference between the lights atop a cell tower a mile away and Venus.
Lesson 3- Use the finder scope and point it at something big. Like the moon. Don’t go looking for Rigel your first time out.
Lesson 4- Realize that the kids are not interested in watching you learn how to do this in real time. They are waiting for you to say – “Hey, come look at this!”
One more pro-tip: Bring a bar stool out to the driveway so they can sit and NOT TOUCH anything on the telescope. As soon as they bump it you have to start all over. And they run back in to play Mario and you are left alone in the cold again. Straining to see the light.
Its amazing how visible light is if you are looking for it. Our universe is mostly darkness (much like our hearts). Rigel (Orion the Hunter’s right foot) is 860 light years away- but even I can find it if I look.
So maybe I have another 2021 candidate motto: Straining to See the Light.
Maybe what we are experiencing now is much like ancient Jews experienced during the Intertestamental period (the hundreds of years between the transmission of Malachi and when John the Baptist showed up telling people to make way for the LORD).
I imagine they had a similar question on their lips- God, where are you? Help us to strain to see the light, Lord. Help us to know the difference between light and dark.
Christmas Lights
So when you don’t go out at all, you look for things you can do in a car. We drive an hour one way to get our goats their shots. Or to deliver duck eggs to a high school friend because she is allergic to chicken eggs. {3}
And this time of year offers a unique opportunity to take a car ride with 4 children under 13 that doesn’t drive you nuts. Just make sure to follow this list:
Everyone goes potty before you head out.
Ensure that you know where the spare house key is, since you don’t really need keys when you don’t go out for 9 months. Getting locked out would probably put a damper on a fun night looking at the lights.
Take your new small dog with you for the ride.
I forgot to mention all the new animals we have gotten. We now have 17 animals:
7 ducks
2 goats (Vincent Van Goat and Mr. Tumnus)
6 chickens (they had names until the kids realized I am serious about eating them once they stop laying eggs)
Dixie, our perfect cat
Doc our new dachshund (sort of)
We got Doc as a birthday present for our youngest. She turned 6, which is of course a big birthday for any kid. But any kid who has a COVID birthday needs something special. Thus, Doc.
I realized in September, with Stacy’s birthday that all my little family- my entire society right now, which honestly is a huge blessing to have this amazing crew as my society- will have at least 1 birthday during this pandemic. With no friends. No eating out. No trips.
Mark was the last one to have a birthday not in quarantine. Mine was first (in April), but I honestly never care about my birthdays. Then Nora’s (when I built the new bedroom). Then Stacy’s (when I built the barn). Then Glory’s – when we got the dog.
Of all things that really rip me up (tore up from the floor up- love that phrase), it’s the impact this has on my kids. And we will turn around soon, and Mark will have his first quarantine birthday.
But anyway. The dog.
Doc is a dachshund-terrier mix. That makes him a derriere.
Thank you for laughing at my joke.
Back to Christmas lights.
We have a gigantic neighborhood less than a mile from us. I mean huge. At least 500 houses are in this thing. And we get lost every single time we go into that beast. Its sort of like a medieval forest upon approach. You enter it with some trepidation, knowing you may not make it back out. But somewhere deep in there is a magical item. Maybe a house made out of candy. Or a lost falcon you need to retrieve. Or a friend you only see once a year. Something that pulls you into the forest.
In this case it was Christmas lights and the attendant accoutrements.
We saw lots of lights. And mostly colored lights. Which is awesome because I love colored lights because they are more real. More of-the-people. The vox populi of lights, if you will (and even if you won’t). Stacy does not like colored lights. But she is starting to see their value. Funny how things you thought you had the luxury of not liking pre-global-pandemic, you start to find a place for them on one of the shelves in your heart.
We saw giant Santas. Some riding elephants (we live in Alabama. But War Eagle!). We saw Snoopy flying his plane. Minions. An entire sidewalk lined with Snowmen lights. Gorgeous green wreaths made of lights. Nativities.
Some yards were meticulous displays of ordered, thoughtful beauty. Some were slapdash menageries of 5 years’ worth of buying whatever Lowe’s or Home Depot had on clearance each year after Christmas was over. It was all magnificent and just what we needed to see that night.
We saw beauty. All made of lights.
But we also got lost.
At one point I heard Nora call out from the back – “hey, you know we have passed this house 3 times now.”
Yes, Nora. I know.
I had thought that if I could get back to the one house I knew (one of Stacy’s dear, dear friends who is fighting cancer during this madness), then from there I could get back out of the forest (this huge neighborhood). Somehow if I could make it back to a place I knew, I could then make it back home.
I was proud that I had navigated back to the friend’s house. But from there I kept getting lost. Going in circles. Hitting lots of dead ends. So many cul-de-sacs. At one point I even recognized the same pile of sticks and leaves I had seen twenty minutes before.
My strategy was not working.
And I did not want to use the normal way of getting back home. The GPS.
But in the end, I had to. And of course, it got us back home (just 1.5 miles away).
I guess all that hit me pretty hard. We were straining for the light. But we were hitting dead ends. We were looking for the beauty. Trying to get back home. But it wasn’t working.
We had to pull out the GPS. I guess when you are lost in the forest, following the breadcrumbs back out may be your very best strategy.
What are our breadcrumbs during this insanity? Have they been stolen by a fairy-tale villain, intent on keeping us lost in the forrest so that the calamity continues and the hopelessness grows?
Coffee cups, widows, fireplaces, and hatred
I am sitting by my fireplace once again this year to write this thing out over the course of probably ten hours and three weeks. Laptop in hand (lap) and coffee cup within reach.
I have a funny thing about coffee cups. I think coffee tastes very different depending on the cup (something about differential heat conduction of materials, or maybe the shape of the rim focuses the heated air rising into my nose a little differently, like different wine glasses or the ones you drink a Stella in). So I end up using 4 or more cups throughout a morning. This drives my wife insane.
In the summertime I will leave them all over the yard as I garden. This also drives my wife insane.
Let’s do one more list for old times sake
First and second cups of coffee (between 4 and 5am)- There is what I call The Porcelain Cup. It’s a thin-walled cup that usually delivers a strong but clear flavor. I usually have my first cup of coffee in this one.
Third cup of coffee- Then there is The Batman Cup. Gifted to me by my youngest son, it is special – but it also carries the boldness of coffee in a more compact taste profile than The Porcelain Cup. I usually have my third cup of coffee in this one.
4th cup of coffee- The Callaway Cup. It is special for 2 reasons: 1 it is shaped like a small terra cotta pot that any gardener instantly recognizes; and 2- we got it on a trip to see Christmas lights with my momma last year, right before The World Changed.
Cups 1 and 2
Cup 3
Cups 4+
Then there is The Daddy Cup.
Its this one. The one I have been showing you different sides of this whole time.
It has 4 Bible verses on the sides of it, each in a different colored rectangle. Each verse explains a key part of the Gospel.
In this sense, this cup really is The Gospel Cup.
It is the one thing of my father’s I have.
And I stole it from Momma. Really just borrowed and never brought it back. But I knew I would never bring it back, so really I stole it.
It has a taste profile similar to The Batman Cup. Strong, bold and compact, and a little off. Like Daddy was.
But lately I have found I avoid drinking from this cup.
I don’t drink coffee in this cup very often anymore. Maybe once every 3 weeks. Maybe.
I think that is for two reasons mostly. The main reason is that it just reminds me so damn much of my father. And when you got to have such an amazing father like I did, and you miss him more with each birthday of your children that passes, or each gray hair you find in your own beard- you just need a break from the aching sometimes.
And he loved coffee. Crappy coffee in my opinion.
He drank it all day long. I think more as a communion with others more than anything else. Some people bond over beers. Or cigarettes. Daddy got into your heart over the course of a cup (or pot) of coffee.
And when I drink from The Daddy Cup, I see him. Very vividly. All his weird facial expressions. All those moments of him lost in thought. And now I see myself with those same expressions. Those same moments of undisclosed thoughts. And in these visions- these memories- I commune with him across the divide of death. In memory I ache.
And during this terrible Dark Night of America’s Soul, I just don’t need another cause of heartache right now. We are all just one more straw away from breaking, and I am no different.
Momma still drives down to the National Cemetery to visit Daddy pretty often.
Nothing will stop that woman from loving that man. Not death. Not COVID. Not bitter cold temperatures. Nor near-breaking-down old cars driven by a 72 year old lady all alone on a country road heading south to see him. Or at least the patch of earth where half of him (his body) lies under a cold stone.
Momma knows the other half (his soul) sits near the Father somewhere.
And that she will sit next to him and laugh again one day. That laugh that you can only have with your partner. Your other half of your One Flesh. The one I still get to have with Stacy each day.
But there is another reason I don’t like to drink out of The Gospel Cup lately.
My heart is so blackened by this past year. By what I have seen from my fellow humans. By what I have seen in myself. Our Total Depravity.
Their ability to convince themselves that the deaths of hundreds of thousands of people are not real. (Or are less important than keeping up their normal lives). {4}
My ability to hate them for it.
I have been changed by this. And not in a good way.
A seething hatred has flooded my heart. And I fear even The Gospel Cup may not break this heart of stone one more time.
I know I should not hate. But I simply cannot see these people the same after seeing their response to all this. I look at them the same way I do people who support abortion. Both groups have convinced themselves the horror is not real. That The Life is not human. Or does not rise to the level of Human needed for change in behavior or policy or law.
But somehow I made my peace with abortionists long ago. Somehow I was able to compartmentalize my disgust at their depraved, evil, acceptance (promotion) of the slaughter of innocents.
I guess I need to figure out a way to put COVID Downplayers and Deniers in that same box. To find a fake, but practical peace. To quarantine their vileness from my eyes so I can pretend to love them again.
I want The Gospel Cup to tear my heart up. To make it beat again. To make it love all my brothers and sisters again.
If anything can do that, The Gospel Cup can. A good cup of coffee in that cup- a communion with my father and my Father- can work wonders. A wonder working power.
Wrapping Up
I just hope we can all listen to this song on New Year’s Eve 2021 and feel its relatable.
I can’t not at least attempt to point you towards some options for hope in all this.
Maybe you need a list.
Maybe you need to burn your fucking lists.
Maybe you need to build something.
Or call an old friend.
Or make a new one over Zoom (it can be done).
Maybe you need some inspiring questions. Here’s 2:
What will you do with the time between now and when this is over?
What will be the first thing you do when this war is over?
Maybe our lives become hybrid mottos of what our fathers passed onto us and what we are now trying to pass on to our children.
If this is the case I guess I am somewhere in between Push on Through and Strain to See the Light. Just maybe I am flying desperately in a rickety early 1900s wooden bi-plane, lost in a dark expanse of clouds, peering frantically with my telescope hanging out of the cockpit- straining to see the light.
Just maybe.
I don’t think I will really know until I can hug my momma again.
Momma holding me, with Aunt Linda staring into my baby face.
And Finally Here is That Blue Butterfly I Promised at The Beginning
If I survived 2020, I can survive anything.
You can too.
Fight against the darkness.
Strain to see the light.
Push through those dark clouds.
FIN
This concludes Clay’s 2020 Year In Review.
Thank you for reading. I love you all.
Love- Clay F.
P.S. There’s more goodies below if you want to check them out.
The Cat Shirt.
A few small Christmas gifts from me to you
And if you made it this far, it means I can trust you with a small box of more goodies.
A pushing thru / straining to see the light playlist
I tried to pull only energetic or encouraging songs (a few darker ones made it through like “Wrecking Ball”, but I wanted even those to have dramatic, cathartic hooks). I spread so much gloom I figured I need to do some penance by giving you something to dance in your underwear to on New Year’s Eve. Its not like anyone is looking this year – so live it up. But if you put this on sometime, do send me a note or text to let me know someone checked this out. It might be a small, small connection that makes us both feel human again.
More Music
He Stopped Loving Her Today
Willie Tribute
7 Bridges Road
The Dance
A prayer for America
Struggling to know how to pray during this time? Try this one-
Dear Heavenly Father,
Whatever is next, prepare us for it.
Give us your strength to survive it and in the surviving not further debase ourselves.
Give us a vision of an America focused on you that does not involve human kings. Release us from the slavery of selfishness. Help us to make truly hard sacrifices.
Hear our prayer!
Dear Jesus,
Please forgive us for what we have done to each other. For our dismissal of all these dead humans you love so much. For evangelism opportunities we squandered.
Please cleanse our blackened hearts. Please forgive us our many sins. Help us to love the Active Shooters.
Dear Holy Spirit,
Please guide our thoughts and our words. Teach us more about The Son. Carry us through whatever is next. Be our Helper. Please!
OUR MISSION We provide a caring, high-quality customer experience to preserve and improve the health and lives of New Yorkers with our integrated healthcare system. OUR VISION To be the number one plan of choice for the communities we serve.
Our Values
• Give care and compassion to all • Be customer powered: Align daily actions to positive, impactful customer experiences, connect with internal and external customers • Be proud of what we do: Take ownership and accountability, be solutions driven • Act as a team: Build trust, empower others, champion transparent communication • Thrive with change: Spark and support innovation, transform our business through technology and data
Culture
Our culture is one committed to quality, because quality allows us to collectively impact lives. OUR WORKFORCE IS OUR MOST VALUABLE ASSET We have built a culture that develops employees professionally and personally. Employees enjoy a familial atmosphere, with open door access to all levels within the organization, and a supportive management team that appreciates the value that each unique individual contributes to the company. Our philosophy is to promote teamwork, collaboration and cooperation throughout our organization, and we are committed to recognize and advance our staff based on their capabilities and performance.
Diversity
WE ARE AS DIVERSE AS THE POPULATIONS WE SERVE. The diversity and culture conversation within our company is a reflection of the same breadth of diversity throughout New York City and the members that we serve. We seek talented, creative individuals from a variety of backgrounds, worldviews and life circumstances to work with us. Developing and retaining our diverse staff is what brings better insights, better decisions, better service and innovation.
Benefits
Generous Time Off Paid vacation, Paid sick leave (so you can take care of yourself and eligible family members when needed most), and a package of up to 11 paid holidays Comprehensive Medical Coverage Plans including MetroPlus Gold, a no cost, no deductible commercial plan exclusively for those employed by New York City Dental and Vision Insurance Plan Employee Assistance Program Financial and savings benefits: 529 college savings plan, Flexible spending account programs, NYC Municipal Credit Union savings program, Employees qualify for Public Interest Loan Forgiveness, Licensure reimbursement, Transit benefit programs, Direct deposit Retirement and pension plans: NYC Employees’ Retirement System (NYCERS) Pension Plan, NYC Deferred Compensation Plan (DCP), 401 (k) and 457 plan, Health + Hospitals Tax Deferred Annuity (TDA) Program 403(b) plan, New York State Voluntary Defined Contribution Program (VDC), Financial wellness programs EMPLOYEE DISCOUNT OFFERS: Our staff members can access discounts for a variety of products, services, and entertainment, including: • Apple and Dell products • Cell phones and mobile plans • Gym memberships • Special discount pricing on sporting events, Broadway plays, concerts, movie tickets, travel packages, and other offers through Barclays Center, Plum Benefits, Perks@Work and Working Advantage ADDITIONAL BENEFITS *These benefits include some or all of the following options: -Disability Insurance -Life Insurance -Health Club Reimbursement -Supplemental Hospital Coverage -Tuition Reimbursement
Professional Development
We support professional development and growth, and the opportunity for all our staff to reach their highest levels of personal potential and team success. GET THE TRAINING YOU NEED TO ADVANCE Take advantage of various training opportunities in classroom and online settings Refresh or learn new technical or leadership skills Apply for full or partial graduate degree scholarships through the Mayor’s Graduate Scholarship Program
Why Join Us?
Because, we are woven into the fabric of New York City Joining our team means contributing to a New York City legacy of quality, affordability, innovation, and service that spans three decades Because, we care about you as a person Here, you’re truly part of the MetroPlus family. We treat our people the way we expect our people to treat our customers Because, we care about your growth We invest in our employees by providing them with extensive professional development opportunities, thus, enabling them to further their professional growth and achieve what they aspire to achieve Because, we care about your health and well-being That’s why we offer an excellent benefits package to every member of our team Because, we do work with real purpose We represent your values












 For whatever weird reason, I have almost no distinction between my work and my life. Clients seem to like it because it makes healthcare consulting human. And genuine human-ness is loved by anyone remotely human. So clients become friends.
For whatever weird reason, I have almost no distinction between my work and my life. Clients seem to like it because it makes healthcare consulting human. And genuine human-ness is loved by anyone remotely human. So clients become friends.